


Nathan Seltzer is a postdoctoral scholar in the UC Berkeley Department of Demography. He received his PhD in sociology from the University of Wisconsin-Madison, where he also trained in demography at the Center for Demography and Ecology. His research explores the relationship between economic change and population trends. In published and ongoing work, he investigates how the decline of the American manufacturing sector has impacted fertility rates, mortality rates, and economic mobility.
Social Science Matrix content curator Julia Sizek interviewed Seltzer about his recent research, using images from his article, “The economic underpinnings of the drug epidemic,” which was published in Social Science and Medicine – Population Health in December 2020. (Please note that captions have been revised for this article.)
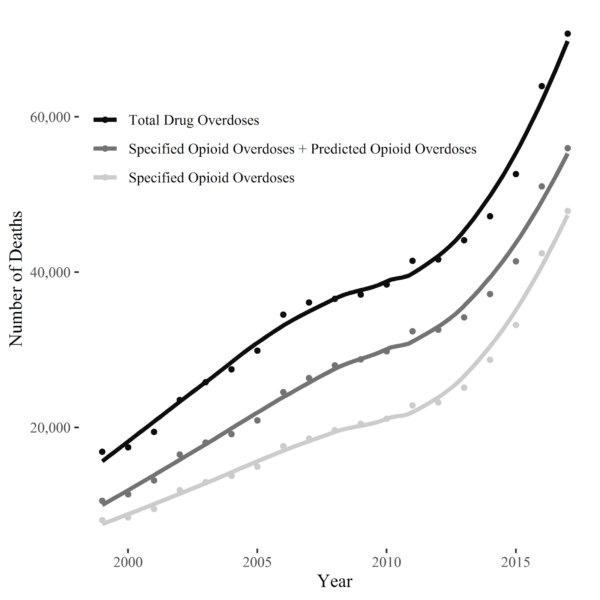
During the last 20 years, the number of opioid-related deaths has been dramatically increasing, as Figure 1 shows. How have scholars typically understood the causes of the opioid epidemic?
There are a number of reasons why drug and opioid overdose deaths have increased over the past two decades. To begin, pharmaceutical companies began ramping up the manufacturing and distribution of prescription opioids in the 1990s. Foremost, Purdue Pharma is known for its role in pushing OxyContin, but the widespread adoption of prescription opioids for pain ailments extends to the broader pharmaceutical industry, which promoted the idea that opioids were non-addictive and safe to use with minimal risks.
The deliberate distribution of prescription opioids by pharmaceutical companies is a supply explanation for what propelled the opioid epidemic. At the same time, we know that supply cannot exist without demand. Recent academic literature, including my study, has found that the success of the pharmaceutical companies in distributing prescription opioids was driven in part by below-par social and economic conditions. In particular, economists Anne Case and Angus Deaton have emphasized in their research how deteriorating quality of life and economic “despair” have proliferated in recent decades. Indeed, there is a strong correlation between measures of economic precarity and opioid prescribing patterns.
While the drug epidemic was initially spurred by the over-prescription of opioid medications, two additional developments kept it going. First, the rise of heroin supply started at the beginning of the 2010s. Second, the rise of synthetic opioids, such as fentanyl, started shortly after the rise of heroin. Yet, the drug epidemic is wider than just opioid use – there has also been an increase in deaths involving psychostimulants and cocaine. In my research, I focus on the broader drug epidemic, rather than just the opioid epidemic, to call attention to this broader development.
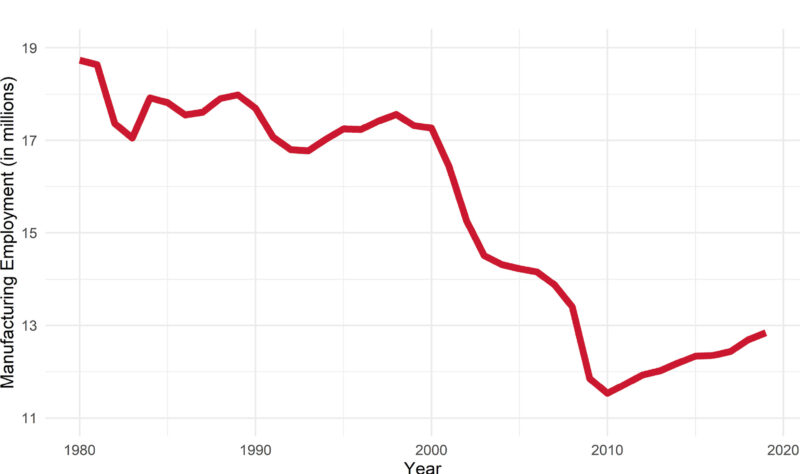
Your research examines the link between the labor market and opioid overdose mortality. In the graph above (Figure 2), we can see the general decline in the number of workers employed in manufacturing. How do scholars normally explain the link between this decline in jobs in the manufacturing sector and opioid deaths, and what is important about manufacturing-sector jobs compared to other declining industries?
The decline of U.S. manufacturing is one of the most important labor market events of the past fifty years. Between 1970 and today, manufacturing jobs went from representing a quarter to less than a tenth of all jobs in the U.S. The issue with this decline is that manufacturing jobs have traditionally functioned as a ladder for upward economic mobility, especially for those without a college degree. As manufacturing employment has decreased, no other industry has taken manufacturing’s place to provide a similar ladder for upward economic mobility. Instead, most employment growth has been in the “low-skill” service sector, which provides wages that are not comparable to those commanded by manufacturing workers.
Scholars have recently begun to examine how these sorts of labor market changes are impacting different facets of society, including trends in drug overdose mortality rates. My research builds on this new literature by examining how the loss of manufacturing jobs predicted the rise of the drug epidemic. The mechanism behind this association is that manufacturing decline heightens economic uncertainty for both workers who are directly laid off, as well as the broader community that experiences reduced employment opportunities. This economic uncertainty fosters a risk environment that increases the likelihood of substance use.

As we can see in Figure 3 (above), there is significant variation across states in the extent to which manufacturing declined. What does examining the opioid epidemic at the state scale show us that’s less visible at other scales, and what did you find when you examined smaller scales at the county level?
I chose the state scale for the primary analysis because there is substantial variation in both drug overdose deaths and manufacturing employment across states. This state-level variation is not just random noise, but the result of different social, economic, and health policies that have been implemented by states over the course of decades. These policies range from labor deregulation to Naloxone access laws (Naloxone is a drug that immediately reverses an opioid overdose) and the creation of prescription drug monitoring programs. Accordingly, population health outcomes are now increasingly determined by state-level policies and regulations, and it is important to take into account these broader socio-political policy regimes when conducting a statistical analysis.
The results of the state-level analysis indicate that states with higher levels of manufacturing employment had lower rates of drug overdose deaths. Specifically, for every one percentage point increment in manufacturing employment, there is a 3.2% reduction in drug overdose rates for women and a 4.7% reduction in drug overdose mortality rates for men. Between 1999-2017 (the length of the study period), the overall decline in manufacturing employment experienced by all states accounted for approximately 92,000 overdose deaths for men and up to 44,000 overdose deaths for women.
In addition to the state scale, I examined whether the association between manufacturing employment and drug overdose deaths held at smaller geographic levels, including the commuting zone level (a level slightly larger than a metropolitan statistical area) and the county level. The results demonstrate that the statistically significant association remains, although the effect size attenuates slightly. This attenuation can be explained by the effects of shifting to a smaller level of geography: by studying a commuting zone or county level on its own, spillover effects, like work commuting patterns across counties, are ignored.

These maps in Figure 4 show the percentage of drug deaths you were able to predict using your model that factored in manufacturing decline. How were you able to use the data from a decline in manufacturing jobs to predict opioid deaths? What were some of the challenges of trying to put together this predictive model, and what were you able to find in terms of the predictive power of manufacturing decline on opioid-related deaths?
The findings of my study indicate that up to 92,000 overdose deaths for men and up to 44,000 overdose deaths for women are attributable to the decline in manufacturing jobs between 1999-2017. These total figures represent the percentage of all drug deaths that are predicted by manufacturing employment levels in each state. As you can see in the maps, the share of drug deaths that are predicted by manufacturing decline varies considerably across state contexts, as well as by sex. I derived these figures using data on the overall percentage point decline in manufacturing employment for each state and data from the estimated statistical models.
The biggest challenge of this project was assembling a dataset that combined data on drug overdose mortality rates with data on manufacturing employment, as well as other social, economic, and policy variables. Assembling this unique dataset allowed me to statistically adjust the models for important alternate explanations other than manufacturing decline that might better explain the rise of drug overdose deaths. To generate mortality rates, I combined data on state-level populations with restricted-use death certificate records from the National Center for Health Statistics at the CDC. For manufacturing employment levels, I worked with data from the Census Bureau’s County Business Patterns program. I then accessed data from various other sources, including the Current Population Survey, the Census Bureau’s Local Area Unemployment Statistics program, and a database on prescription drug policies. Including variables in the model from all of these individual datasets improved the theoretical and methodological rigor of the research.
What racial and gender differences did you find in your model?
Much of the previous literature on the opioid and drug epidemic has focused on middle-aged white males because they initially had the highest levels of drug and alcohol usage in the 2000s in comparison to other race and sex groups. In my research, I sought to examine whether the effect of manufacturing decline on drug overdose deaths was generalizable to other population subgroups. Generally, the effect remains the largest for middle-aged white males between the ages of 45-54, but the effect is also large for adult white males of other ages, as well as for adult white females of all ages. For Black males and females, the effect is generally not statistically significant, but there are important exceptions: manufacturing decline was associated with drug overdose deaths for Black females ages 45-54 and Black males ages 35-44 and 55-64. These findings go against the widespread, but unfounded notion that manufacturing decline has primarily impacted white male workers. In fact, as evidenced by William Julius Wilson’s research, Black workers experienced substantial losses in manufacturing employment over the course of the final two decades of the 20th century.
What are some of the implications of your research for policymakers and institutions?
This paper speaks to a growing literature that finds a relationship between social conditions and the rise of the opioid and drug epidemic. The implications of the results – that higher manufacturing employment is associated with lower rates of drug overdose deaths – signal the importance of policy interventions that aim to reduce persistent economic precarity experienced by individuals and communities, especially the economic strain placed upon the middle class. We live in a world where it is unlikely that major growth will occur in the U.S. manufacturing industry; however, an emphasis on improving jobs in the service sector should be the focus. Improvements in wages, benefits, and job stability in the low-wage service sector might decrease economic uncertainty and therefore provide a pathway toward reducing drug and opioid overdose mortality.


